Results
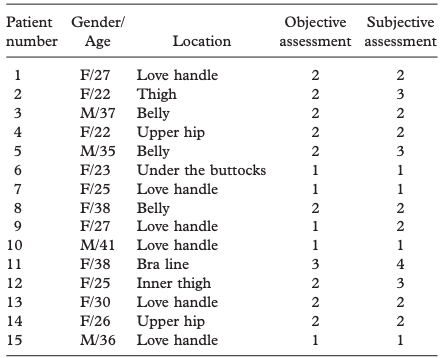
Initially, 18 patients volunteered to participate in the study; however, 3 patients were conclusively excluded from the study due to loss to follow-up. The reason for loss to follow-up was not related to results of the procedure, such as unsatisfactory outcomes or complications, and was due to personal affairs. A total of 15 patients (11 women and 4 men) fulfilled all of the requirements of the investigation. The mean age was 30.1 years, with a range of 22 to 41. Treatments were delivered primarily to the love handles (40.0%, n=6), belly (20.0%, n=3), upper hip (13.3%,n=2), inner thigh (13.3%, n=2), bra line (6.7%, n=1), and under the buttocks (6.7%, n=1). Patient information and assessment outcomes are described in Table I.
The treatments delivered to different anatomic sites were also analyzed by gender. Men almost exclusively received treatment to the love handles (50.0%, n=2) and belly (50.0%, n=2). Women, in comparison, received treatment over a much wider range of areas, including the love handles (36.4%, n=4), upper hip (18.2%, n=2), inner thigh (18.2%, n=2), bra line (9.1%, n=1), belly (9.1%, n=1), and under the buttocks (9.1%, n=1). The treatment sites were also analyzed by patient age range. The patients were divided into 2 groups, 20 to 29 years old and more than 30 years old. The number of patients in each group was similar, with 8 for the former and 7 for the latter; however, the composition was quite different. The treatment sites of the former group were love handles (37.5%, n=3), upper hip (25.0%, n=2), inner thigh (25.0%, n=2), and banana muffin (12.5%, n=1). The latter group received treatments of the love handles (42.9%, n=3), belly (42.9%, n=3), and bra line (14.3%, n=1). It can be assumed that both groups were interested in treatment of the love handles, but the younger group desired modification of the thigh or hip area and the older group was more concerned with their belly.
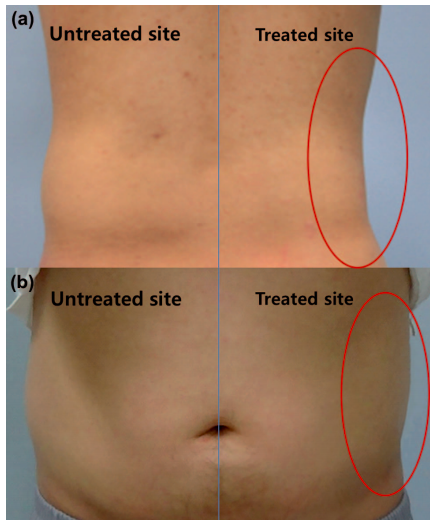
Results of both the objective and subjective assessments were revealed to be statistically significant (p < 0.05) compared to the baseline state. The average point of the objective assessment was 1.7, which implies good to excellent improvement or 50% to 100% subcutaneous fat reduction. The average of the subjective assessment was 2.1, indicating moderately satisfactory results. The assessments were also analyzed by gender and treatment site. The average values of the objective and subjective assessments of male patients were 1.5 and 1.8, respectively. The average points for female subjects were 1.8 and 2.2, respectively. It seemed that the male patients showed slightly more favorable results with cryolipolysis than their female counterparts. The most satisfactory treatment site was area under the buttocks, followed by the love handle. The average values for the objective and subjective assessments of under the buttocks were 1.0 and 1.0, and the love handle showed points of 1.3 and 1.5, respectively. Clinical photos of love handle treatment by cryolipolysis are described in Figure 1. The male patients received cryolipolysis treatment once on the right and once on the left love handle area. After 3 months, they all showed excellent improvement and expressed significant satisfaction with the results. The most dissatisfactory area was the bra line followed by the inner thigh. The average values for both the objective and subjective assessments of the bra line were 3.0 and 4.0, respectively, and the values for the inner thigh were 2.0 and 3.0, respectively.
Each subject was closely observed and managed for possible complications during the entire course of the study. All patients experienced immediate erythema (Figure 2a) and minor pain for several hours, but these symptoms vanished within one day without specific management. Bruising (Figure 2b) emerged in some patients at the treatment site and disappeared within 2 to 5 days without further treatment. Neurologic complications, such as tenderness, dulling of sensation or numbness, or tingling sensation, were not reported until 3 months after the last procedure. All patients were also shown to have no other long-lasting symptoms or discomfort at the last questionnaire 3 months after the last treatment.